What is the definition of HFpEF in medical terms?
HFpEF - Heart failure with reduced ejection fraction
Heart failure with reduced ejection fraction (Heart failure with preserved ejection fraction (HFpEF) is a clinical syndrome in which patients have signs and symptoms of heart failure as the result of high left ventricular (LV) filling pressure, despite normal or near-normal LV ejection fraction (LVEF; ≥50 percent).




|
Related read: HFpEF and HFrEF are complex conditions often requiring different modes of detection and therapy. Our article, HFpEF vs HFrEF, goes into greater detail about both the similarities and differences between them. It covers the structural, molecular, and cellular mechanisms that contribute to HFpEF and HFrEF, and the other key differences in their risk factors, diagnosis, and treatment. |


|
Related read: Our article, Diagnosing Heart Failure with Preserved Ejection Fraction, goes into greater detail about how HFpEF is diagnosed according to current clinical guidelines; including history and physical examination, imaging via rest and stress, natriuretic peptides, staging, and new integrated approaches. |
How is artificial intelligence supporting HFpEF diagnosis?
Radical progress is being made
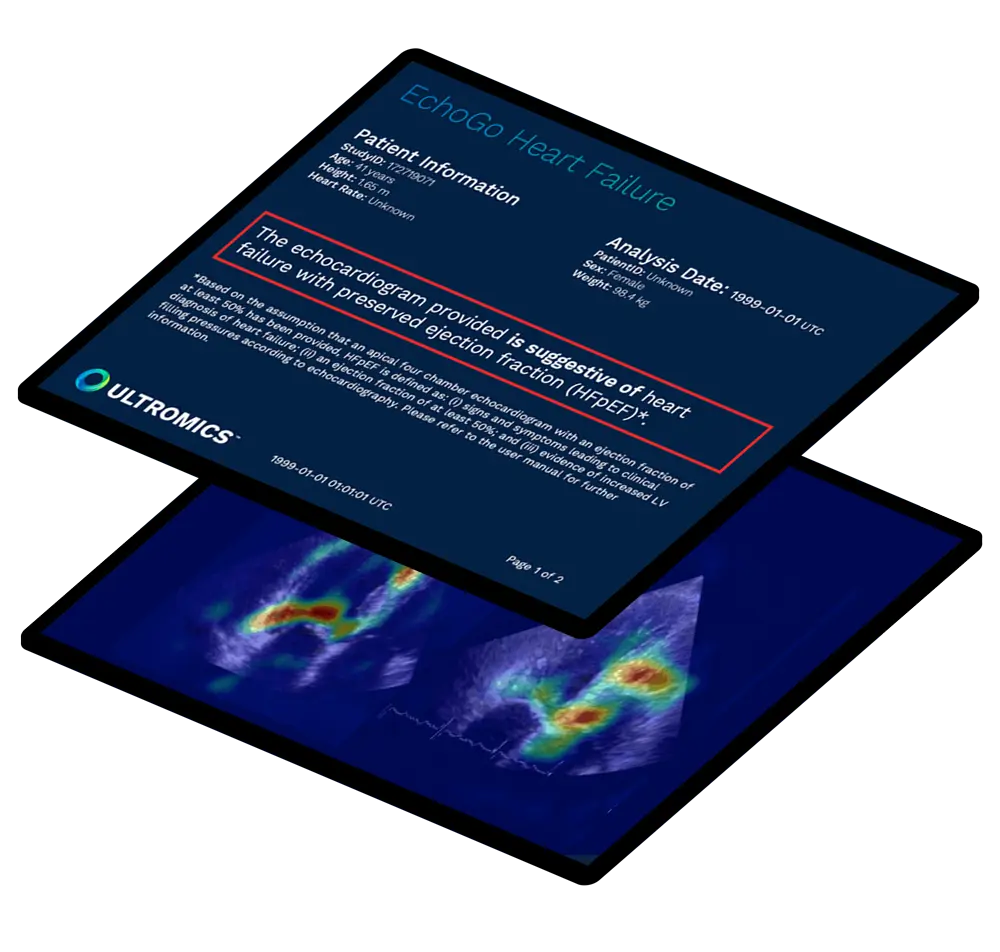
There is an urgent need to develop precise tools to help diagnose HFpEF patients so they can receive faster access to life-saving new treatment. EchoGo Heart Failure, from Oxford University and built in collaboration with the Mayo Clinic, delivers precision HFpEF detection using the power of AI from a single apical 4-chamber view of an echocardiogram.
The AI in EchoGo Heart Failure can be applied for HFpEF and marks a huge leap forward from traditional diagnostic algorithms for HFpEF.
74%
of cases correctly reclassified that were otherwise indeterminate.
How can HFpEF be treated?
Treatment
To date, the exact mechanisms and effective treatment strategies for HFpEF are still poorly understood. Therapy has largely been focused on the management of symptoms and comorbidities, such as medications to lower blood sugar in diabetic patients. Evidence published in the EMPOROR-PRESERVED trial shows sodium-glucose cotransporter 2 inhibitors (SGLT2is) are the first drug class to improve cardiovascular outcomes in HFpEF. [10] Recommended in the 2022 HF guidelines, SGLT2is have demonstrated a relative risk reduction in heart failure hospitalizations by 29%. [11]
29% reduced risk of hospitalization
In addition to results published in the EMPOROR-PRESERVED trial. The DELIVER trial for another SGLT2i Dapagliflozin showed a reduction in worsening heart failure which included any of:
- An unplanned hospitalization for heart failure
- An urgent visit for heart failure
- Cardiovascular death
Results found Dapagliflozin reduced the rates of these end points versus the placebo.
16.4% Dapagliflozin
19.5% Placebo

Envisioning a better outlook for HFpEF patients
Partners supporting HFpEF detection
The National Institutes of Health (NIH) and the National Heart Lung and Blood Institute (NHLBI), managed by the Foundation for the National Institutes of Health (FNIH), have come together with key partners such as Ultromics to form The Accelerating Medicines Partnership® Heart Failure (AMP® HF).
The 5-year, $37 million multi-stakeholder collaboration brings together partners from both public and private sectors across the world to investigate HFpEF.
This partnership comes in response to the overwhelming need to better understand HFpEF.
Frequently asked questions (FAQs)
You can find more information about complete and ongoing trials with AI for HFpEF on our Clinical Trials Proof page.